MIBG Scan
Page Content
Indications:
Neuroblastoma
Phaeochromocytoma / Paragangliomas
Principle:
Preparation and Procedure:
The patient should not have a bone scan less than 2 days before or until 5 days after the Iodine-123 MIBG injection. A GFR study should not be performed until at least 6 days after the Iodine-123 MIBG injection.
The patient must not have either CT with oral contrast or a Barium study less than 5 days before the Iodine-123 MIBG injection or until after imaging has finished (usually 26 hours after the injection). These x-ray studies will interfere with MIBG scanning.
Lugol's Iodine (thyroid blocking agent) needs to be started 1 day before the Iodine-123 MIBG injection and should be continued for 3 days. 1 or 2 drops to be taken daily in milk.
Foods such as chocolate (including chocolate milk), can block the uptake of MIBG. They must be avoided for 4 days before the MIBG scan.
Certain drugs interfere with MIBG uptake and should be avoided (usually for 3 biological half-lives): Decongestants and nasal sprays, Tricyclic Antidepressants, Antipsychotics/Tranquillisers, Amphetamines, Antihypertensives.
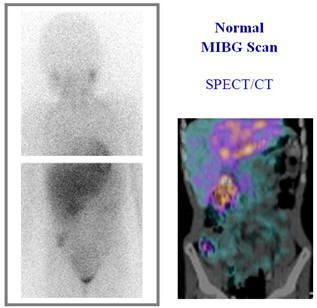
MIBG imaging takes about 1.5 hours (including SPECT/CT). Infants and children with neuroblastoma will often need sedation or anaesthesia.
Comments:
MIBG is an expensive investigation and requires a lot of organisation between departments and the suppliers of the radiopharmaceutical. At least 2 week's notice is usually required to arrange the study. Currently the Iodine-123 MIBG arrives and is injected on Tuesdays. The imaging is performed 24 hours later i.e. Wednesdays.
MIBG sensitivity in the detection of neuroblastoma has been reported to be 90% or greater, specificity approaches 100%. The extent of metastatic bone and bone marrow disease is most accurately defined by MIBG scintigraphy however small liver mets may escape detection due to the high concentration of MIBG in the liver. The accurate depiction of the full extent of disease spread and distribution are essential before therapy for both prognostic classification and therapeutic decisions.
MIBG sensitivity for pheochromocytomas is 80% and specificity 95-99%. CT and MRI are accurate in detecting primary tumours of the adrenal gland but they are inferior to MIBG in the detection of extra adrenal tumours.